|
a |
|
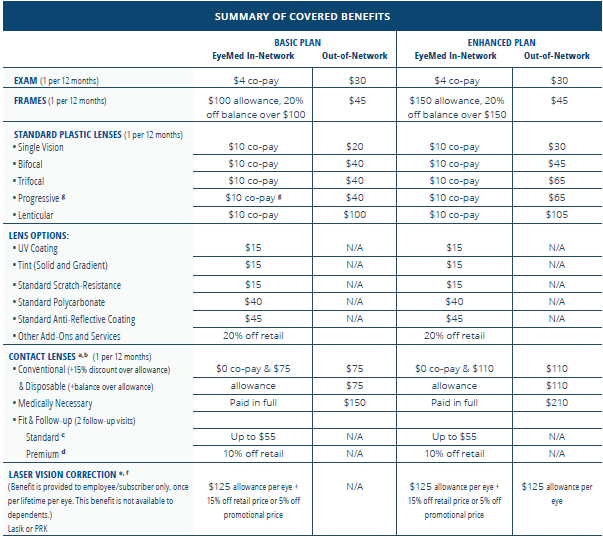
Contact Lenses in lieu of eyeglass lenses |
|
b |
|
Contact Lens allowance is a one-time use allowance per benefit year |
|
c |
|
Standard Contact Lens Fitting-spherical clear contact lenses in conventional wear and planned replacement |
|
|
|
(Examples include but not limited to disposable, frequent replacement, etc.) |
|
d |
|
Premium Contact Lens Fitting-all lens designs, materials and specialty fittings other than the Standard Contact Lenses (Examples include toric, multifocal, etc.) |
|
e |
|
Laser vision benefit in lieu of all other covered benefits |
|
f |
|
Members receive discount from the U.S. Laser Network, owned and operated by LCA Vision. |
|
g |
|
Progressive lenses under the Basic Plan are covered with co-pay and 80% of charge less $120.00 allowance. |
Summary of Limitations & Exclusions
|
This plan will not cover:
|
- Orthoptic or vision training, subnormal vision aids, and any associated supplemental testing
- Medical and/or surgical treatment of the eye, eyes, or supporting structures
- Services provided as a result of any Worker’s Compensation law
- Benefit is not available on certain frame brands in which the manufacturer imposes a no discount policy
- Corrective eyewear required by an employer as a condition of employment, and safety eyewear unless specifically covered under plan
- Plano non-prescription lenses and non-prescription sunglasses (except for 20% discount)
- Services or materials provided by any other group benefit providing for vision care
- Two pairs of glasses in lieu of bifocals
- Aniseikonic lenses
- Services received before your effective date, including started but not completed services
|
Louisiana State benefit enrollment and termination rules apply. Contact your benefits administrator for details.